TECH SHEET · 1295.DAC · GHRHR AGONIST
A precision GHRH analog, engineered for a seven-day half-life.
Four protective residue substitutions, a covalent albumin tether, a single Phase 1 dose-escalation, and a halted Phase 2 program. The CJC-1295 evidence base, read as engineering spec.
The short version
CJC-1295 is a synthetic peptide designed to trigger the pituitary gland to release growth hormone. It was engineered to last far longer than the natural signal it mimics — the original hormone clears the bloodstream in about seven minutes, while the CJC-1295 DAC form (the version with a covalent albumin-binding modification) stays active for five to eight days. That extended duration is the molecule's central design achievement.
One small Phase 1 study in 22 healthy adults documented the pharmacokinetics and confirmed the hormone response. A Phase 2 trial intended to test its effects on body composition was discontinued before reporting results. No approved human indication exists. CJC-1295 is a research chemical — not an approved drug, not a compound pharmacy can legally fill, and prohibited at all times in competitive sport under WADA rules.
Research communities report effects ranging from improved sleep and faster recovery to water retention and blood-sugar shifts. Those reports are anecdotal and not from controlled trials. The full breakdown of what people report is on the effects page. The published science is on the research page.
Section 01 — Compound
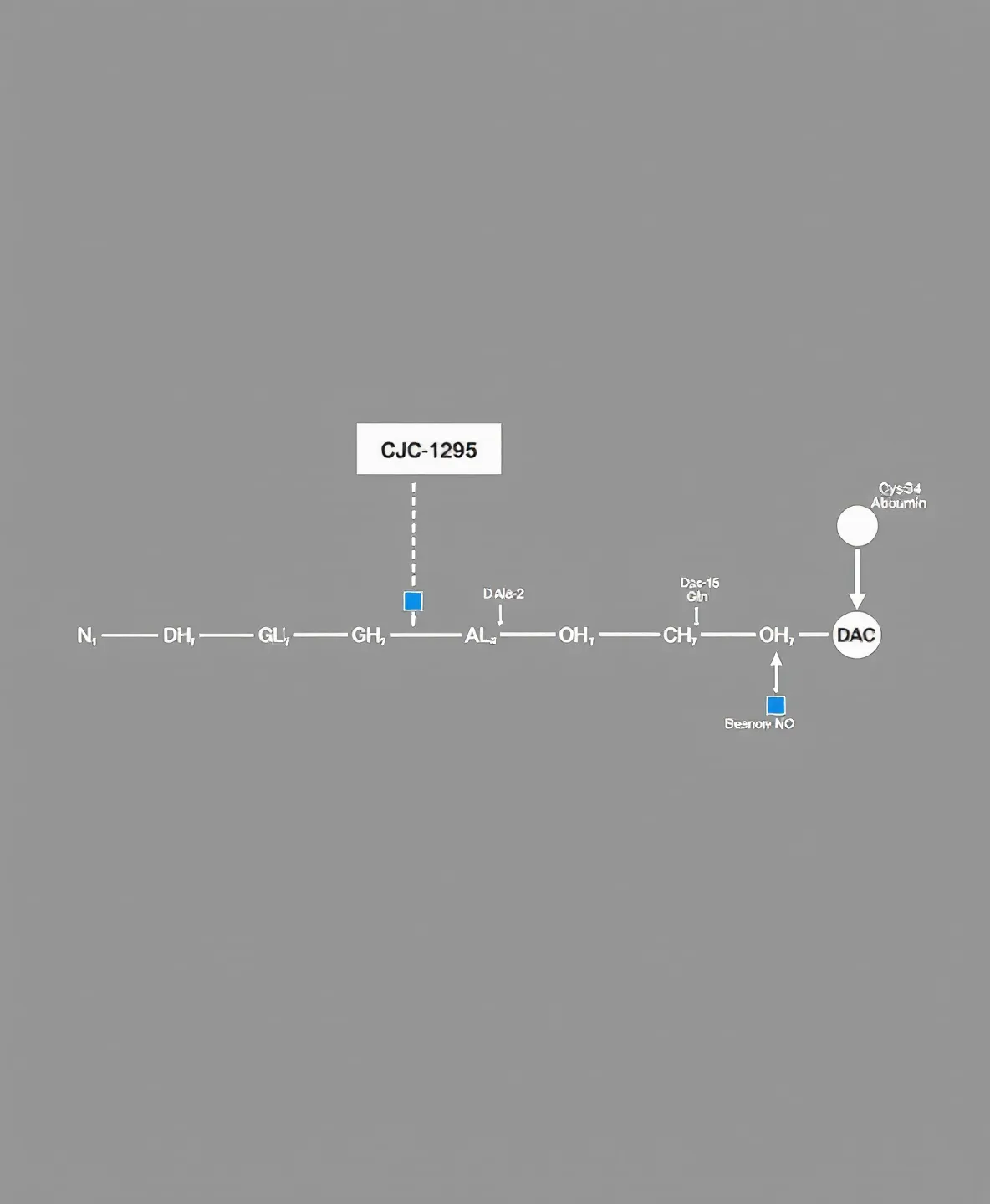
CJC-1295 is a 30-residue synthetic peptide derived from human growth hormone-releasing hormone (GHRH). The backbone is the first 29 amino acids of native hGRF, modified at four positions — D-alanine at position 2, glutamine at position 8, alanine at position 15, and leucine at position 27. Each substitution closes a specific proteolytic vulnerability: position 2 resists dipeptidyl peptidase-4 cleavage, position 8 resists deamidation, position 15 resists trypsin-like proteolysis, and position 27 resists oxidative damage [1].
A 30th residue carries the Drug Affinity Complex (DAC) modification — an N-epsilon-maleimidopropionic acid group that undergoes a Michael addition with the free thiol of cysteine-34 on circulating serum albumin. The product is a covalent peptide-albumin bioconjugate roughly 70 kDa in apparent mass [1]. This single chemical step is what converts a peptide with a native half-life measured in minutes into a peptide with a plasma half-life measured in days.
The non-DAC backbone, sometimes labeled modified GRF(1-29), retains the four amino acid substitutions but lacks the maleimide. Its half-life sits at approximately 30 minutes — a roughly 4-fold extension over native GHRH but two orders of magnitude shorter than the DAC variant. Conflation between the two molecules in lay and vendor literature is endemic; they are pharmacologically distinct.
Section 02 — Mechanism
The receptor target is the growth hormone-releasing hormone receptor (GHRHR), a class B G-protein-coupled receptor expressed on anterior pituitary somatotrophs. Receptor engagement triggers a Gs / adenylyl cyclase / cAMP / PKA signaling cascade that drives CREB-mediated transcription of the GH1 gene and the release of stored growth hormone [5]. Downstream hepatic IGF-1 (somatomedin C) production amplifies and biomarks the signal.
The 2020 cryo-electron microscopy structure of the GHRHR-GHRH-Gs complex (PDB 7CZ5, 2.6 Å resolution) showed that GHRH binds as a continuous α-helix engaging all three receptor extracellular loops, the extracellular domain, and every transmembrane helix except TM4 [5]. The structural picture explains atomistically why the four CJC-1295 substitutions preserve receptor activation while resisting peptidase attack — none of the modified residues participates directly in the receptor-binding interface.
A mechanistic point recurs across the recent endocrinology literature: GHRHR agonism produces robust GH stimulation that does not exceed physiological pulse limits, because IGF-1 negative feedback at the hypothalamus continues to regulate peak amplitude even when the GHRH input is sustained [14]. This distinguishes GHRH-axis activation from direct exogenous recombinant GH administration.
Section 03 — Pharmacokinetics
The pivotal human pharmacokinetic data come from a single Phase 1 dose-escalation study in 22 healthy adults aged 21-46 years [2]. Single subcutaneous doses of 30, 60, 125, and 250 μg/kg produced mean plasma GH elevations of 2- to 10-fold over baseline persisting at least 6 days, and mean IGF-I elevations of 1.5- to 3-fold persisting 9-11 days. Multiple-dose cohorts maintained IGF-1 elevation for up to 28 days after the final dose. Mean plasma half-life across the dose range fell at 5.8-8.1 days.
A substudy of the same cohort examined whether the multi-day pharmacodynamic profile abolished endogenous GH pulsatility. It did not: trough GH rose approximately 7.5-fold while the discrete pulse architecture — pulse number, amplitude variability, inter-pulse interval — remained intact [3]. Mean GH rose 46% above baseline. The structural picture is a raised floor with the pulses still firing on top, not a flat plateau.
The 2009 proteomic substudy identified five candidate serum biomarkers of CJC-1295 dosing — apolipoprotein A1 and transthyretin isoforms reduced, β-hemoglobin and an albumin C-terminal fragment and immunoglobulin fragments increased, with the immunoglobulin/albumin spot correlating linearly with IGF-1 [6]. The proteomic signature is the most granular dosing readout in the published human record.
Section 04 — Clinical development
The sponsor-funded clinical program halted in October 2006. A Phase 2 randomized double-blind trial of CJC-1295 in HIV-associated visceral adiposity (NCT00267527, n=192) terminated after a participant death from an acute coronary event approximately two hours after the 11th weekly dose [8]. An independent review attributed the event to pre-existing undiagnosed coronary artery disease and judged it unrelated to study drug, but the primary efficacy endpoints were never published in peer review and no sponsor-funded clinical development has resumed.
The class-effect benchmark for visceral-fat efficacy comes from a structurally related FDA-approved GHRH analog, tesamorelin: 15-20% reduction in visceral adipose tissue over 26 weeks of daily 2 mg subcutaneous dosing in HIV-associated lipodystrophy [11]. The CJC-1295 Phase 2 program was originally designed against this benchmark; whether it would have hit it remains untested.
A separate randomized trial of tesamorelin in older adults (NCT00257712, the SMART study, n=152, 20 weeks of daily 1 mg SC) produced significant improvement on executive function (P=0.005), a positive trend on verbal memory (P=0.08), 117% IGF-1 elevation, and 7.4% reduction in body fat [9]. This is the strongest class-level evidence that pituitary GHRH-axis activation can yield measurable cognitive effects in older adults — a research signal, not a license to extrapolate to CJC-1295 dosing in any human population.
Section 05 — Regulatory chassis
CJC-1295 is not approved for any human therapeutic indication by FDA, EMA, or any other major regulator. On September 20, 2024, the FDA removed CJC-1295 from Category 2 of the interim 503A bulk drug substances list after the original nominators withdrew their nominations [16]. The action unwound the September 2023 'do not compound' designation that had been in place for roughly a year; it did not constitute approval. CJC-1295 remains a research chemical and remains outside legitimate compounding-pharmacy practice.
The World Anti-Doping Code 2025 Prohibited List reaffirms CJC-1295 under Section S2 — Peptide Hormones, Growth Factors, Related Substances and Mimetics — as prohibited at all times, both in-competition and out-of-competition, for any athlete subject to WADA testing [17]. The analytical chassis that supports enforcement is recent: a 2021 metabolism paper characterized 19 in vitro metabolites of CJC-1295 and validated an LC-MS/MS detection method at limits at or below 1 ng/mL in urine [12], and a 2024 nano-LC Orbitrap method validation [15] formalized the routine-testing pipeline.
Forensic identification of seized illicit CJC-1295 in the gray market was confirmed by high-resolution LC-MS/MS sequence determination in 2010 [13]. Counterfeit and impure 'research chemical' CJC-1295 has circulated since; product identity, purity, sterility, and endotoxin burden in non-pharmaceutical channels are not assured.